Daniel
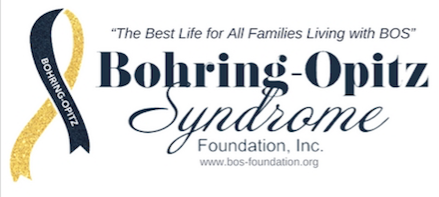
DANIEL LUKE: His Journey with Bohring-Opitz Syndrome
By: Lori Fulton Cutillo
March 4, 2019

Upon his birth by elective C-Section on July 23, 1999, Daniel Luke Cutillo surprised everyone with his relatively small size (6 lbs. 8 oz.) His brother had been 3 lbs. heavier at birth. Additionally, Daniel looked unusual. He had a red birthmark on his forehead, almost no fingernail on his right index finger, and “overlapping toes,” (middle toes underneath the others). Nevertheless, at birth and in the newborn period, Daniel fed well, and seemed healthy.
By about 2 months, however, Daniel’s condition appeared worrisome. He had poor eye contact and was socially delayed. He had developed severe reflux, and vomited virtually every feeding (a condition he would have for 10 years or more). And, his growth was poor---not even measurable on the growth charts. We took him to a geneticist who ran the standard chromosomal battery. When the test came back normal, the geneticist proclaimed Daniel free from genetic defects.
Unfortunately, the geneticist’s reassurance was short-lived. At 4 months, Daniel’s pediatrician learned that he had lost the recently acquired ability to roll over. Daniel was also lying on the examination table lifeless and motionless. The pediatrician made an urgent referral to both neurology and genetics at Children’s Memorial Hospital in Chicago.
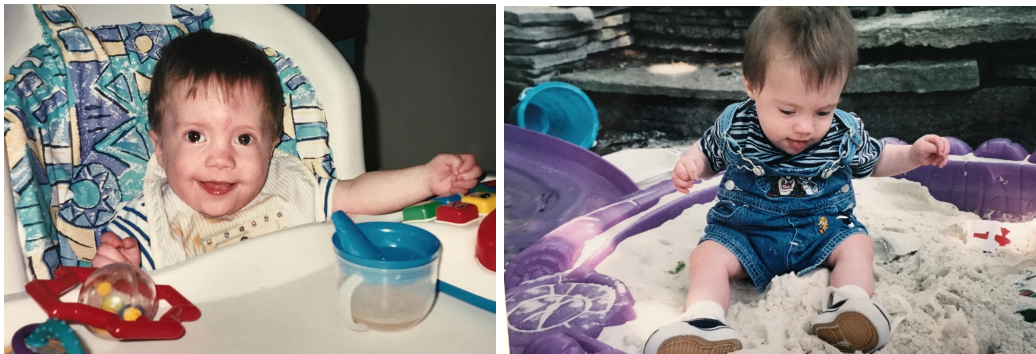
Although the neurology consult was normal, the geneticist indicated that Daniel did, in fact, have a genetic disease or syndrome. She began an exhaustive work-up. Meanwhile, by mid-infancy, Daniel had developed recurrent ear infections (he later received ear tubes). He was also diagnosed with high myopia and began wearing glasses. Developmentally, he was globally delayed, and began to receive services in OT, PT, SLT and later cognition. He sat up on his own for the first time at 9 months (in the sandbox pictured above).
The Children’s Hospital geneticist revealed additional dysmorphic features of which we had been unaware. In addition to the birthmark, hypoplastic fingernail and overlapping toes, Daniel had low set and posterially rotated ears, anteverted nares, depressed nasal bridge, high arched central palate and he held his fingers in an overlapping position. All of that and he still looked adorable!

When Daniel was about 15 months old, his geneticist informed us that in part due to Daniel’s poor growth and feeding, and the genetic testing’s negative results thus far, she felt he should be evaluated for a mitochondrial disease. We took Daniel to a preeminent mitochondrial disease specialist who performed a fresh muscle biopsy. According to that testing, Daniel had oxidative phosphorylation defects in Complexes I and IV of the respiratory chain. The doctor indicated that Daniel’s presentation fit mitochondrial disease and dismissed his dysmorphic features as nonspecific. We had our answer . . . or so we thought. For the next 17 years, Daniel’s doctors accepted as accurate Daniel’s mitochondrial disease diagnosis.
After a period of relative calm, Daniel’s 10th-12th years brought several new medical problems. First, he was diagnosed with a borderline prolonged QT interval (a minor heart arrhythmia). He also had a grand mal seizure. Daniel recovered from the seizure in the hospital and while there, underwent an MRI. The MRI revealed that he had a lesion in the mid brain/pontine junction. This indicated that at some point, Daniel had suffered a stroke. About a year later, Daniel had a sleep study that revealed severe obstructive sleep apnea (resolved by removing adenoids and tonsils). Daniel also had an EEG with rather dramatic results (but uncertain implications). His EEG revealed epileptic encephalopathy with nearly 100% slow-wave sleep occupied by spike wave discharges. Finally, we learned that Daniel had severe joint contractures, with both kneecaps dislocated. The orthopedist indicated that nothing could be done for the kneecaps—he would need to live that way (and he has).

During this time (middle childhood), Daniel continued to demonstrate severe developmental disabilities. He played with infant toys, and watched Barney and Sesame Street. He adored his older brother, and scooted all over the house to find entertaining things. Without exaggeration, Daniel was always smiling and happy. He had no behavioral problems of any sort.
About the time Daniel turned 14, he entered the most distressing and painful period of his life. Out of the blue, he began banging his head hard on walls and hitting himself in the face and eyes. Shocked by this behavior, we sought help from his neurologist and his complex care physician, who hospitalized him for several days. The doctors’ consensus (and ours’) was that Daniel was experiencing pain of uncertain etiology. They did not feel it was a behavioral phenomenon. Pain drugs were tried, and Daniel responded well to Gabapentin and Topamax, drugs that can be helpful for headaches. His neurologist gave him the diagnosis “probable migraine variant.”
The drugs helped, but over time, lost some effectiveness. Daniel continued to hit himself in the face for hours a day. In the Fall of 2014, we received the worst news. Daniel had detached his own retina and had no vision in his left eye. We were dismayed that the medical professionals had not warned us of this possibility—we had not appropriately protected him.
Daniel continued to engage in this self-injurious behavior at various levels for 4 years. Fortunately, we learned how to protect him (with hard arm splints).

At age 18, Daniel went for a routine genetics visit. The geneticist (new to Daniel) questioned Daniel’s mitochondrial disease diagnosis. He pointed to the fact that Daniel had suffered no disease progression, and also noted Daniel’s many dysmorphic features, which did not necessarily preclude mitochondrial disease, but also were not typical of it. The geneticist asked us to submit to Whole Exome Sequencing and felt that we would likely learn that that Daniel had a genetic syndrome.
When the testing came back, we finally had an accurate answer as to Daniel’s genetic status. He had Bohring-Opitz Syndrome. It’s important to recognize that Bohring did not even describe the syndrome until the year of Daniel’s birth (1999). It would have been difficult to identify Daniel earlier given the nascent state of research during his childhood.
We also learned that Daniel had not just 1, but 2 genetic mutations. He had the ASXL1 mutation that caused BOS, but he also had a mutation in the MC4R gene, which causes obesity. For the last few years, Daniel had steadily gained weight and become obese (a far cry from the malnourished toddler he had been!) This would explain why he persistently focused on food and never seemed sated. As far as the mitochondrial disease diagnosis, the geneticist indicated that Daniel might have secondary mitochondrial dysfunction, a phenomenon they were seeing in other syndromic children.
It was thrilling to know with certainty in which “camp” Daniel belonged. Right away we reached out to other BOS families who have been lovely. Daniel even looks like his BOS brothers and sisters! And of course, they share many of the same medical and developmental issues.

Daniel is now 19 years old. Developmentally, he functions at the 6 month to 1 year level. He does not walk or talk, but has a few adapted signs he typically uses to request food. He is large—196 lbs.---and wears diapers. Lifting Daniel is a challenge, but we have wonderful long-term caregivers who help him. Daniel loves music, soft books, and sparkly lights. His favorite day is his wonderful school’s semi-formal dance.
Raising a child with severe disabilities presents a parent with physical, intellectual and emotional challenges. It is easy to fall into nonproductive thinking. Why us? Why him? Like most of life’s difficulties, answers are elusive. What can you count on? Your special child will bring you abundant innocent and unadulterated joy. He will adore you and your other children just as you adore him. He will touch others and make a difference in their lives. And, he will strip away the unnecessary and highlight the most important elements in your life. Your child will teach you about love.